A brief history of conversion “therapy”
Understanding the history of the anti-LGBTQ practice and why it must be opposed at all costs.
Work in progress Last updated: February 2026
Across the country, bills have been introduced with various strategies all aimed at accomplishing the goal of promoting the long-discredited, dangerous practice of conversion therapy. In Spring 2023, Wisconsin debated AB3/SB4, which would enjoin the state licensing boards for social workers and marriage and family therapists from prohibiting licensees from engaging in what is otherwise known in the field as Sexual Orientation (SOCE) and Gender Identity Change Efforts (GICE). This exists in sharp contravention to the direction the fields of mental health and medicine have taken, and represent deeply troubling developments.
In 2009, the American Psychological Association formally came out against SOCE in a policy (updated 2021) which correctly established that not only are SOCEs hugely immoral and unethical, they’re dangerous and ineffective. Sexual Orientation and Gender Identity are innate characteristics that, while they may organically shift in expression and identification over time, do not respond to psychological or therapeutic intervention. More to the point, nor should they, and nor should anyone ever be induced to be someone who they are not.
Despite the abundance of efforts stretching back a century to change LGBTQ persons (or “convert” them to heterosexual and cisgender persons), no credible evidence has ever been found to suggest that such practices are effective. In the extremely small number of cases where practitioners have claimed success, the effects are transitory, and leave in their wake elevated rates of substance abuse, depression and suicide — both ideation and attempts. They are quite literally deadly.
At present, the practice is opposed by every major professional organization in the United States in mental health and medicine. The United Nations defines conversion therapy as a form of torture, and licensing boards have increasingly held that such practices are serious enough to warrant loss of licensure. Yet despite this, there are still places where conversion therapists practice and at present, actors predominately within the Republican party in the United States are hoping to bring them back, and exempt them from legal scrutiny and protect providers of such care torture from disciplinary action.

Content Warning:
The following resource is offered for those seeking to understand the history of conversion therapy as a practice, why it is banned, and why it is essential to oppose any efforts whatsoever that might seek to lift such bans. While the information is provided in a factual manner, the facts themselves are quite upsetting. Please use caution before continuing.
Historical background: the history of “inversion”
Historically, there have been several types of conversion therapy that have used disparate methodologies aimed at specific demographics.
As noted in this blog post, early conversion therapy at the the turn of the 20th century focused largely on gay men and people assigned male at birth who somehow were perceived as transgressing male gender roles in a way that required “correction”. Unlike today, where anti-gay therapeutic aims are considered unethical and in fact grounds for a therapists’ disbarment, in 1910 the idea that someone would want to “cure homosexuality” was seen as an obvious one. Although people debate ferociously about whether or not Freud actually saw being gay as a problem, he certainly treated it as one. Freud tackled it early on, with his theory of “sexual inversion”. Freudian understandings of human sexuality were based on drives, which propelled the ego to pursue the “object” of sexual attraction. This heavily male-centric picture of sexuality painted sex as a pursuit, and assumed that attraction was based on a third-party that was not the self. The worldview of early psychoanalysts reflected the narrow frame in which people were seen to operate: sexual attraction was a heterosexual pursuit built into the human experience with the function of perpetuating the species by building in an inherent and unceasing pursuit of sex and procreation.
In fact, sex was so central to Freudian theory that Freud based his entire framework of child development on psychosexual stages, which are designated periods in a person’s development where specific foci such as the urogenital system or the pursuit of sexual pleasure dominate even early development. In an ironic display of narcissism, psychoanalysts projected their own experiences of sex as being universal. They then saw digressions from this presumed-universal experience as being the origins of all of what was then called “deviant” sexual and gender behavior.
Since Freud equated maleness and male heterosexuality with normality, even women’s sexuality as a whole was seen as a byproduct of men’s attraction. By this, Freud believed that female sexuality was in the desire to be pursued, to make oneself desirable as a mate and therefore mother. Women who did not desire children were seen as inherently abnormal, and women who did not desire children but were forced to have them anyway were seen as the ultimate villains in an awful lot of origin stories.
From the above lens, where human beings allegedly all desire procreation, heterosexuality is seen as the anchor upon which human development rests, and serves as the motivation both conscious and otherwise, for all actions. Those perceived to be men, therefore, who eschewed traditional masculinity or did not wish to express their masculinity in a way that was considered conventional were seen as disordered. When asked to explain the disorder, Freud stated that since in early sexual development the sexual object is identified outside the self towards the “opposite” sex, it stood to reason (in Freud’s mind) that those who pursued people of the same sex or gender had this backwards. He explained this a handful of ways, but ultimately it was believed that sexuality was turned “back inwards” and “towards the self”. This explanation also became the grounds for the alleged association of homosexuality and transsexuality with narcissism. This last talking point has again become popular among modern-day analysts like Joe Burgo, whose work with Genspect to “treat gender dysphoria” relies on the assumption that people who transition do so in an act of ultimate selfishness.
Freud’s exact position on sexual orientation is actually more difficult to pin down, but the idea stuck. Psychiatrists attempting to “treat” gay men, typically against their will, did so by exploring maternal relationships under the assumption that “psychic wounds” sustained during early childhood laid the foundation for same-sex attraction. While this idea would fall out of favor in mainstream psychology with the depathologization of homosexuality, it remains in the practices of contemporary conversion therapists like David Pickup.
Despite the emphasis on homosexuality, the theory of inversion was applied equally to transgender women and gender non-conforming boys. Publications in psychiatric journals which alleged to “treat cross-gender behavior” often included both gay men and transgender women regardless of sexual orientation, as at the time psychiatry didn’t view the two things as being all that different. In fact, the majority of psychiatrists saw cross-dressing and even “cross-gender identification” (non-cisgender gender identity) as being different ends of a spectrum of non-normative behavior. Up until recently, the very same methods were used for both.
“History is littered with the destruction resulting from the "treatment" of unusual sexual interests and the assumption that there is a "normal" erotic target location… …Individuals with these interests were incarcerated, killed, shunned, committed to asylums, labeled as mentally ill, or forced to undergo "treatment."
Elaborate psychiatric theories were created to imply a scientific basis for, and to justify the oppression of, individuals with different erotic interests.”
— Charles Moser, 2009
The 1950’s & “aversion therapy”
While the majority of etiological (origin-based) explanations used to justify conversion therapy have rested in psychoanalysis, one particularly bleak period in this history involves no insight-oriented psychotherapy at all, but is in fact based in behaviorism. In the 1950’s well through the 1980’s, behaviorists used what is known as “Aversion Therapy” to treat a number of conditions, as well as to attempt to “rehabilitate” a variety of socially unsanctioned behaviors and identities. This was particularly true for young children who displayed gender non-normative behaviors, including children who were gay and/or those who identified with genders incongruous with their sex assigned at birth.
Based on B.F. Skinner’s theory of operant conditioning, in which Skinner observed that co-occurring feelings and stimuli can shape a person’s behavior even in the absence of verbal reinforcement, aversion therapy pairs negative sensations (such as revulsion, disgust or fear) with stimuli thought to be arousing.
We now know that what Skinner observed was based off of what’s called Hebb’s Principal, which you may have heard as “cells that fire together, wire together”. Our brains contain complex networks of smaller networks of neurons which accomplish specific tasks. As the brain matures, these collections of neurons are connected via synapses, which allow complex tasks to be built from slightly simpler tasks, the way you might think of a function in a computer program.
Hebb’s principle also means that if, for instance, that if you feel an emotion at the same time something is happening, that emotion may become linked in your brain to whatever that thing is. The utility of this is not restricted to behaviorism. Modern trauma therapies like EMDR rely on Hebb’s Principal to pair soothing cognitions with traumatic memories, instilling a sense of safety where safety was otherwise taken. By pairing this with a neutral stimulus such as a blinking light or a vibrating device, associations are undone while others are rerouted or built anew.
The 1970’s and behavioral modification.
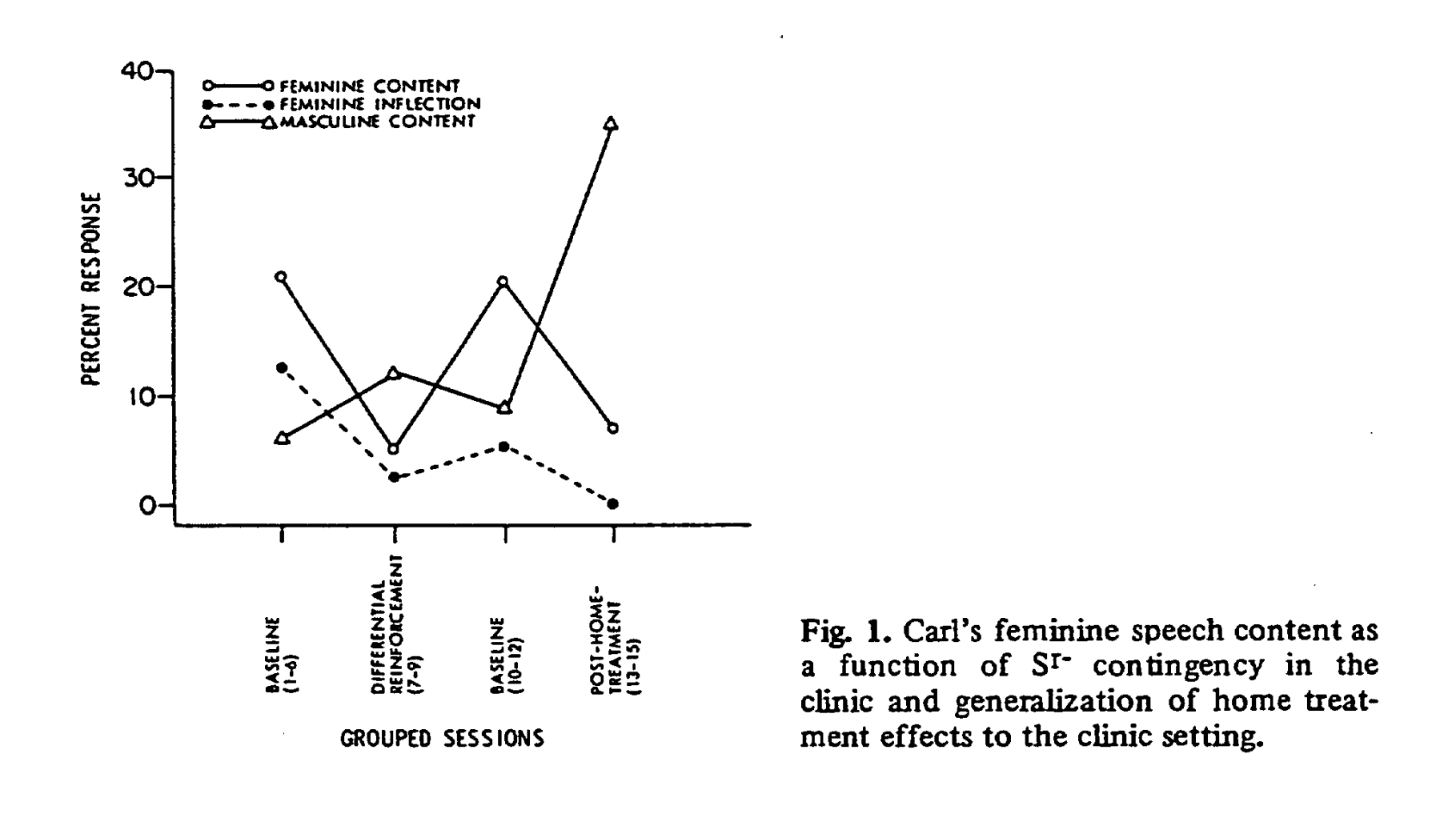
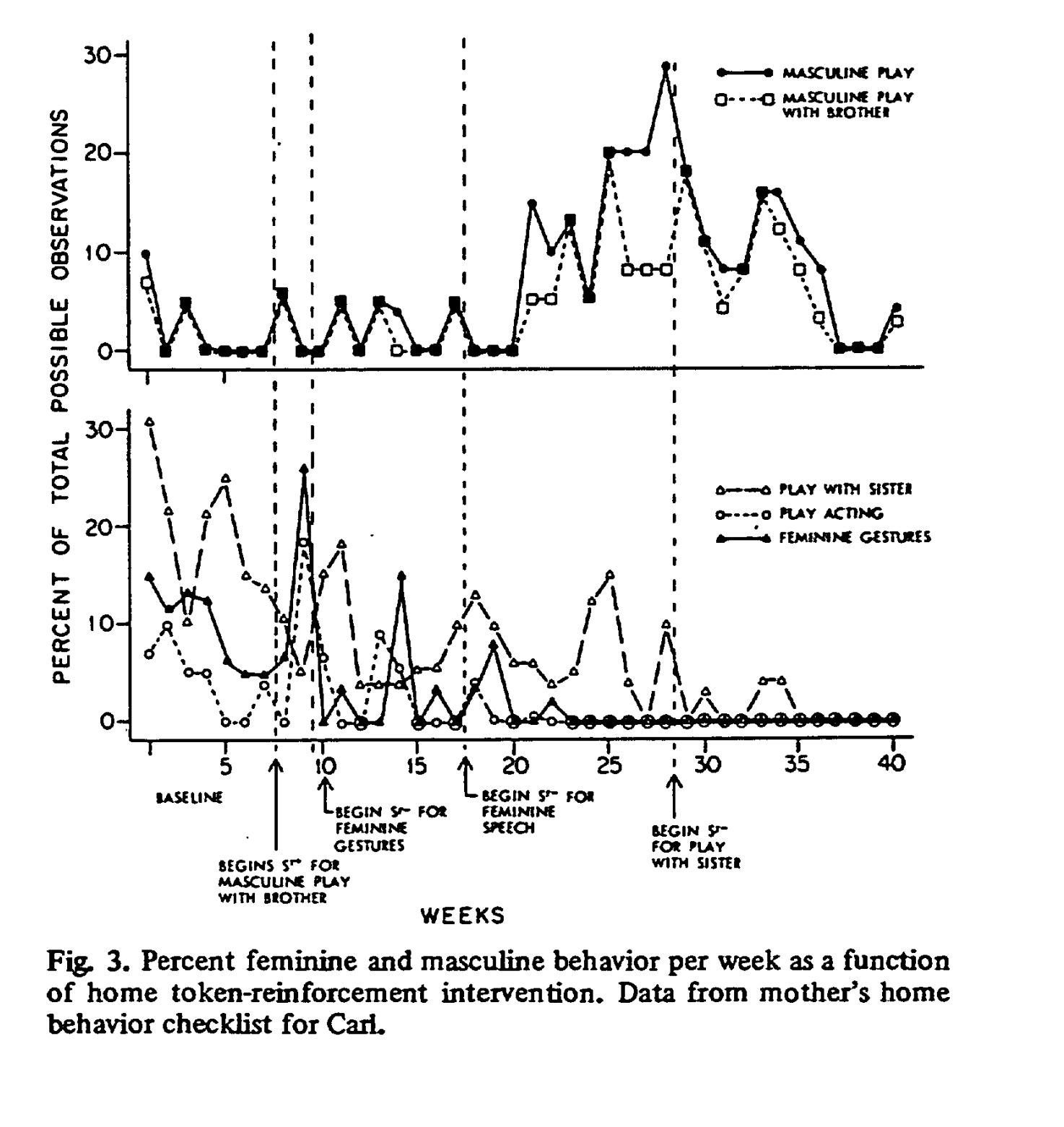
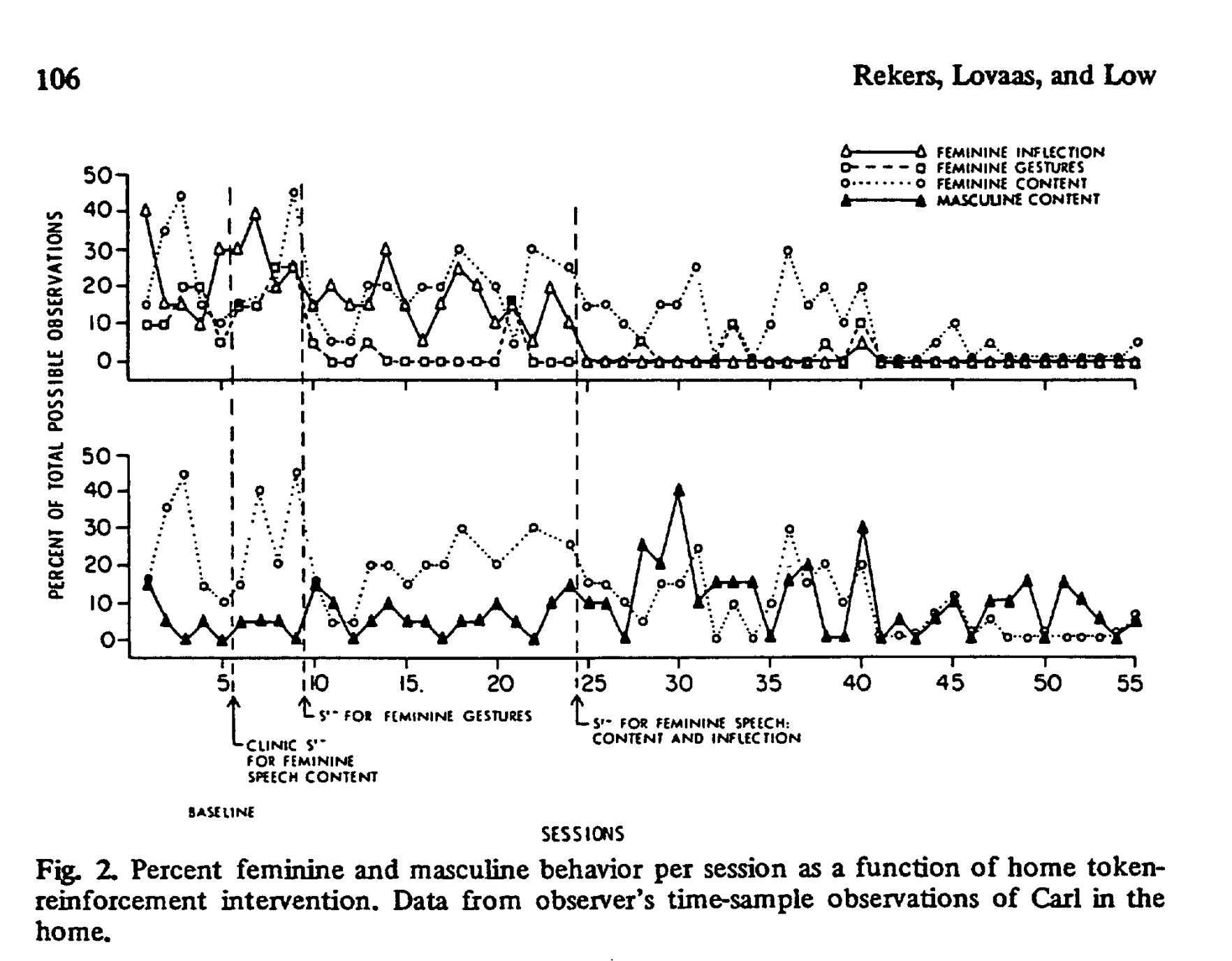
Behaviorists also targeted children, with particular animosity for those assigned male at birth perceived to be “feminine”. In a now infamous paper by Rekers, Lovaas & Low (1974) in the Journal of Abnormal Child Psychology, an 8-year-old child assigned male at birth is cruelly subjected to behavioral conditioning in all aspects of their life, including at school where teachers were coached on how to use negative conditioning to dissuade the child from behaviors considered “too feminine”. A detailed log was kept by researchers at all times to track the child’s behaviors, the charts of which they proudly and heartbreakingly published in the body of the journal.
History: the Church
It is impossible to understand the landscape of conversion therapy, especially within the United States, without first examining the role of the church in the provision of basic services throughout the country. Starting with the “charity care” movement, through adoption and foster care, hospice care and marriage counseling, many of the most important services that people might need throughout their lives are only consistently offered by religious institutions.
This is in part because faith offers a centralized framework for how we move through life. For people of faith, the question is often less about what one desires for themselves and more about God’s plan. Faith institutions operate services as “ministries”— services which meet specific needs in the lives of certain populations, while bringing people “closer to God” through proximity to other people of faith.
While the United States bills itself as a secular country most of the time, our collective refusal as a society to fund social services outside of that which is mandated by law leaves many aspects of life totally without coverage. And while this offers a way for faith institutions to offer helpful and sometimes necessary services to people in need like food banks, it also opens the door for unregulated practices which, in areas like behavioral health, can be quite harmful.
Much of mental health counseling in the US is actually provided by pastoral counselors. Pastoral counseling is performed by clergy, and while much of what is provided as pastoral counseling is deeply meaningful for those within faith communities, it is also a legal gray area for practitioners who wish to circumvent licensing boards. As it pertains specifically to conversion therapy, it typically involves a surrender to God and an atonement for one’s perceived sins. These practices center around the idea that if one prays hard enough, God will take away unwanted attraction or cross-gender identification and be “saved”. While there are many programs around the country which do offer secular mental health training to would-be clergy, such as dual-degree MSW/MDiv programs, far more clergy-based programs offer no clinical training at all, and many churches do not consider formal training to be a necessary element of pastoral development. Provided you preach within a denomination with open enough rules, anyone who opens a church can provide pastoral counseling regardless of training.
While professional counseling organizations have long-banned conversion therapy, pastoral counseling occupies a bizarre liminal space that’s difficult to regulate in a country so emphatic on Christian religious freedom. Bible colleges like Liberty University or Bob Hope University offer a place where religiously-motivated practitioners can hang a shingle without the potential ire of the licensing board. In the United States, while it’s illegal to practice medicine without a license, psychotherapy is a little less clear. The various disciplines that practice psychotherapy (eg., psychologists, social workers, licensed marriage and family therapists and licensed mental health counselors) each have their own governing bodies, and separate from these are licensing boards that operate as quasi-state institutions regulating practice.
While states require licensure and registration, only those who wish to work within the formal medical system technically need to do so. The advent of quasi-disciplines without formal oversight like life coaches have allowed people without clinical training or licensure to accept payment for the provision of a service that may appear quite similar to real, evidence-driven behavioral health care. And while insurance companies will not reimburse for life coaches or pastoral counselors without formal licenses, this is not true of many practitioners who have both. The baffling nature of the US healthcare system means that people seeking care cannot always tell what type of provider they’re seeing using easy heuristics you might rely on in other countries. This is especially true in the case of relationships and sexuality counseling, which only have very limited reimbursement under most health plans.
The merger of the church and the clinic has produced a canon of clinically questionable materials, particularly under the language of “unwanted same-sex attraction” (see below) that straddles the line confusingly between the clinical and theological. Shirley Cox, a clinical social worker who received the awards from the Nevada chapter of the National Association of Social Workers in 1991 and 1992 did the majority of her work in conversion therapy. She is one of 7 authors of the “Understanding Same-Sex Attraction: where to turn and how to help” for the Church of Jesus Christ and Latter Day Saints. Despite the fact that many of authors are clinically trained, the book is replete with anti-gay sentiment and is written entirely from the point of view that being LGBTQ is a sin against God to be overcome through prayer. Despite Cox’s notoriety and open embrace of conversion therapy, NASW has never acknowledged their role in Cox’s career, nor did they take any steps to curb her access to the halls of power in the area as a representative of social workers everywhere. She went on to become President of NARTH, discussed below, as well as to advise some of the first gender-affirming care bans in the United States (see: Kant & Boskey, 2023).

When “homosexuality” was removed from the DSM in 1980 and replaced with “ego-dystonic homosexuality”, it was done so not because of secular scholarship but at the behest of religious organizations like Exodus International. The use of the word “dystonic” refers to a concept from Ego Psychology, where distress is caused by going against the self. The function of this new diagnosis was to allow some providers to continue to treat “unwanted same-sex attraction”— the preferred parlance of homophobic organizations, without running technically afoul of the increasing consensus of professional health organizations that conversion therapy was dangerous and deadly. Groups with ties to both the secular world and the religious pastoral care world like the National Alliance for the Research and Treatment of Homosexuality (NARTH) formed to further muddy these waters .
A “right to treatment”?
One of the biggest battlegrounds between the 1970’s and mid-1980’s was an attempt by homophobic practitioners within both the secular and non-secular spheres to assert that one has the “right to treatment”. Queerphobic organizations argued that consenting patients should have the right to be rid of same sex attraction, and that it is a breach of patient autonomy to prevent access.
In what should feel like a clear mirror to today’s discourse around the rights of transgender, nonbinary and gender-diverse people, detractors within psychiatry and the clinical disciplines argued that the move to depathologize LGBTQ people came not from science, but from the radical Gay Liberation Movement. Critics claimed that patients should have the right to rid themselves of something which so obviously came with a lifetime of stigma and social ostracization. Of course this misses two things: ostracization and stigma are issues with society, not queerness, and there has never been empirical evidence that it’s actually possible to change sexual orientation or gender identity.
In reality, since Freud, psychiatry has long believed there was a cause to LGBT identity— and that such a cause, if fully elucidated could be the object of treatment. This is reflected in the work of people like Richard Green, who is perhaps most famous for his book “The Sissy-Boy Syndrome”. Green was far from an outlier, and his work was extremely popular as late as the mid-1980’s, as evidenced by this 1986 article about his book in the New York Times.
Contrary to claims by conservative lawmakers that Conversion Therapy was specific to electric shock, psychologists tried dozens of mainstream modalities to rid patients— willingly and otherwise— of same-sex attraction and cross-gender identification.
Reparative Therapy
As a brand, few specific frameworks for conversion therapy have received as much attention as Joseph Nicolosi’s “Reparative Therapy” model. Reparative therapy is so well-known that it is specifically mentioned by the United Nations and the World Health Organization, and is widely accepted not only as discredited, but extremely harmful.
To Nicolosi being gay was a symptom of a societal and spiritual breakdown which he attributed mostly to the absence of fathers or the presence of what psychodynamic theorists might call “psychic wounds”.
Despite Nicolosi’s failure to produce evidence of this theory, his book on the subject spread like wildfire due to his affiliation with powerful Evangelical and Catholic organizations. That doesn’t mean, however, it was received well by the rest of the field. Archives of Sexual Behavior, the subject of recent and frequent controversy, featured a review from Richard Friedman MD is severely critical, and notes a paucity of contemporary (for the time, meaning the early 1990's) evidence. Friedman points out that Nicolosi is clearly overtly hostile to the prospect of someone being gay, and writes that “it is unfortunate that Nicolosi, who seeks to be a spokesperson for the legitimate needs of these patients, has published a book with grave clinical, scientific, and scholarly limitations.”
Nevertheless, thanks in part due to the spread of groups like NARTH, of which Nicolosi was a founding member, Reparative Therapy spread widely. It was celebrated and lauded in particular by “ex gay” groups which claimed to united people who wished to overcome “unwanted same-sex attraction”. After Nicolosi died in 2017, Reparative Therapy was rebranded by his son, who calls it “Reintegrative Therapy” and is adamant that this new version is nothing like the old. While practitioners of Reparative Therapy may be shy about using the name given how clearly psychotherapy organizations have condemned the practice, it is visible in any narrative which alleges to link trauma to LGBTQ identity. It has served as a critical influence groups like the American College of Pediatricians who worked closely with Nicolosi throughout the the past two decades up until his death. For an extraordinary breakdown of the sordid history of Reparative Therapy, do yourself a favor and check out “Quacks”, a detailed report and timeline from the Southern Poverty Law Center.
The reemergence of the Jungians & “Gender Exploratory” Therapy
While psychoanalysis has never strayed too far from its anti-LGBTQ roots, the rest of the psychotherapy world largely has. In the past fifteen years, however, certain facets of the psychotherapy world have clung to the past by bringing back old ideas as new frameworks. This has been most apparent in the secularization of frameworks like Reparative Therapy under the guise of Jungian psychoanalysis. While Jung himself was iffy on Christianity, he believed that by looking to mythology we could unlock secrets of the human experience that might give insight for clients into their lives. Although he had been a student of Freud’s, he and Freud disagreed on several fundamental elements— most notably about the structure of the tripartite self. Jung’s embrace of dramatic changes in behavior and self-identification as defense mechanisms gave rise to the widely-rejected theory of Rapid Onset Gender Dysphoria that has become such a gift to the right-wing in both the United States and abroad.
Jung’s belief in the collective unconscious was bolstered by his belief in “psychic epidemics”, later referred to as social contagions. Jungian adherents of this belief system believe that trans identity is the result of trauma or other psychic or moral injury leading to walling off or recasting parts of the self in a different image as a defense mechanism against dealing with the primary sources of pain. They offer no evidence for this, but simply point to the large proportion of psychiatric struggles found within transgender samples as evidence that the two are linked.
Recently, a group of “Gender Exploratory Therapy” practitioners have emerged to practice frameworks primarily rooted in Jungian analysis with the intention of alleviating or “curing” gender dysphoria. They believe, as Nicolosi did, that attending to psychic wounds will eliminate the need for transgender identities. The name was chosen with intention, to imply that other types of psychotherapy ban “exploration” of gender with gender-diverse youth. However, what they claim and what happens in gender clinics every day have very little to do with one another. In reality, the majority of clinics explore gender and what gender means to each patient in depth, providing support and affirmation as they go. This last part, however, is the difference. Practitioners who practice under the banner “Gender Exploratory Therapy” see themselves in opposition to the affirmative model, which is to say that they do not believe trans people when we tell them who we are. To them, trans identity is still identity— many of its practitioners are routinely on record as saying “there is no such thing as a transgender child,” and believe that affirmation will lead to immediate iatrogenic harm. They reject the body of evidence that shows such methods are harmful, and are gaining ground in convincing lawmakers that they have a clinical justification for the elimination of trans rights.
Further reading & resources:
-
Rather than focus on specific types of conversion therapy, the fundamental question parents should ask for their LGBTQ+ child when finding a therapist is whether this is someone who will see them for who they are. This guide talks about how to recognize red flags.
-
Psychology Today is far and away the most popular means for prospective clients and patients finding therapists and prescribers (e.g., psychiatry, PMHNPs, etc). But it has a surprising lack of moderation, and conversion therapists are practicing out in the open. Here’s how to spot them.
-
While by no means authoritative, I’ve compiled this resource based on questions from students and colleagues trying to understand contemporary conversion practices and how they fit into the broader historical landscape. It’s a primer I hope to keep adding to.